
Evidence in the scientific literature suggests that certain minerals and vitamin intakes are deficient in large proportions of Western populations. Essential nutrients that are of particular concern include vitamin D, chromium, calcium and magnesium. The main reason for low intake of certain essential elements is a combination of lowering food quality that excludes whole grain sources of cereals, as well as declining soil quality in many agricultural areas. As a result many individuals choose to supplement with a multivitamin and mineral supplement in order to ensure an adequate intake of essential nutrients. Athletes are one group in which this is particularly true, partly on account of the increased energy intakes associated with hard training that often require high intakes of nutrient poor foods in order to fulfill the energy needs of hard physical activity. Generally, supplementation of athletes with a multivitamin and mineral supplement has been shown to effectively increase levels of some nutrients.
For example researchers1 have investigated the effects of supplementation of a high strength multivitamin and mineral supplement in 22 physically active men for 12 weeks. The contents of the supplement are shown in figure 1. Measurements of blood, urine and 4 day dietary food intakes were taken at baseline as well as at 6 weeks and 12 weeks. During the course of the study, no changes were noted in the blood concentrations of vitamin A, vitamin C and no changes were noted in the status of zinc, calcium or magnesium although the supplement contained over 300% of the RDA of these nutrients. In contrast blood levels and urinary excretion of thiamine, riboflavin, vitamin B6, vitamin B12, pantothenic acid and biotin increased by week 6 and this level was maintained for the remainder of the study. Blood and urinary levels of the B vitamins had returned to baseline values within 1.5 weeks of the end of the supplementation period.
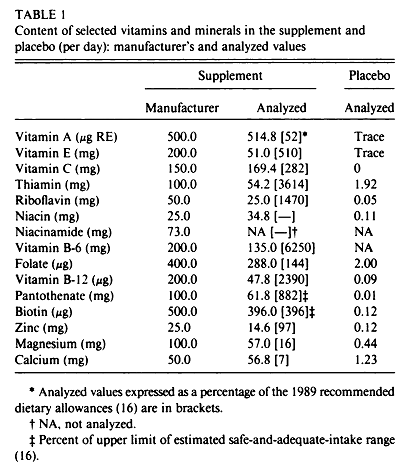
Figure 1. The contents of the multivitamin and multimineral consumed by the athletes.
Surprisingly there are only a handful of studies in the nutritional literature that have looked at the effects of supplementation of a high strength multivitamin and mineral supplement. Of interest in the results of this study are the inability of supplemental vitamin A to raise blood levels of retinol, which has also been reported in other research. This may be because the levels of retinol in the subject were already 2.48 µmol/L which is regarded as adequate blood levels. Similarly vitamin C levels did not rise by supplementation, and this was possibly due to the low amount (120 mg) present in the supplement. The calcium and magnesium levels were also very low in the tablet and the forms of the vitamins may not have been the most absorbable forms of the minerals, although this was not reported. The fact that zinc, calcium and magnesium urinary levels did not rise with supplementation suggests that these minerals were not absorbed, or that levels were too low to affect nutritional status.
Vitamin E levels increased over the course of the study, but this was not significant. Had the study continued the rise may have become significant. Vitamin E is fat soluble and stored in adipose tissue along with triglycerides and other clinical trials have also reported no increase in plasma levels following supplementation. This may also be due to the form of vitamin E given, as synthetic DL-α-tocopherol is not as effective as the natural D-α-tocopherol at raising blood levels. However, there is no indication in the study as to which form of vitamin E is used. In fact this study did not report in detail on the ingredients in the multivitamin, which makes it much harder to interpret the results. As expected levels of the B vitamins increased in plasma and urine significantly following consumption of the supplement. This supports other research investigating the effects of B vitamins that have reported increases in plasma levels on B vitamin with supplementation, particularly those investigating homocysteine.
Dr Robert Barrington’s Nutritional Recommendation: Overall these results show a low efficacy of the multivitamin to effect improvements in the nutritional status of the athletes, with the exception of the B vitamins. This may relate to the short duration of the study or the use of poorly absorbed forms of nutrients. Mineral absorption in particular is dependent of the form of the minerals supplied. Inorganic metal ions tend not to be well absorbed in humans nutrition. Chelating the minerals with organic molecules improves absorption considerably as the organic chelate is recognised by the transporters in the gut and this facilitates bioavailability. The most absorbable forms of minerals and vitamins are found in plants, which is why high quality diets should be used to obtain as many minerals as possible. Synthetic vitamins and inorganic minerals in multivitamins can be used as a ‘supplement’ to a good diet, but should never be a substitute.
RdB